What does an autonomous medical AI agent actually do in an EHR sandbox? → It ingests patient histories, orders diagnostic tests, interprets results, and proposes diagnoses and treatment plans within a simulated FHIR‑compliant environment.
Can AI match physician diagnostic accuracy without human oversight? → In the MIRA study it achieved 88.9% accuracy, slightly above a matched physician cohort, but safety and governance still demand human supervision.
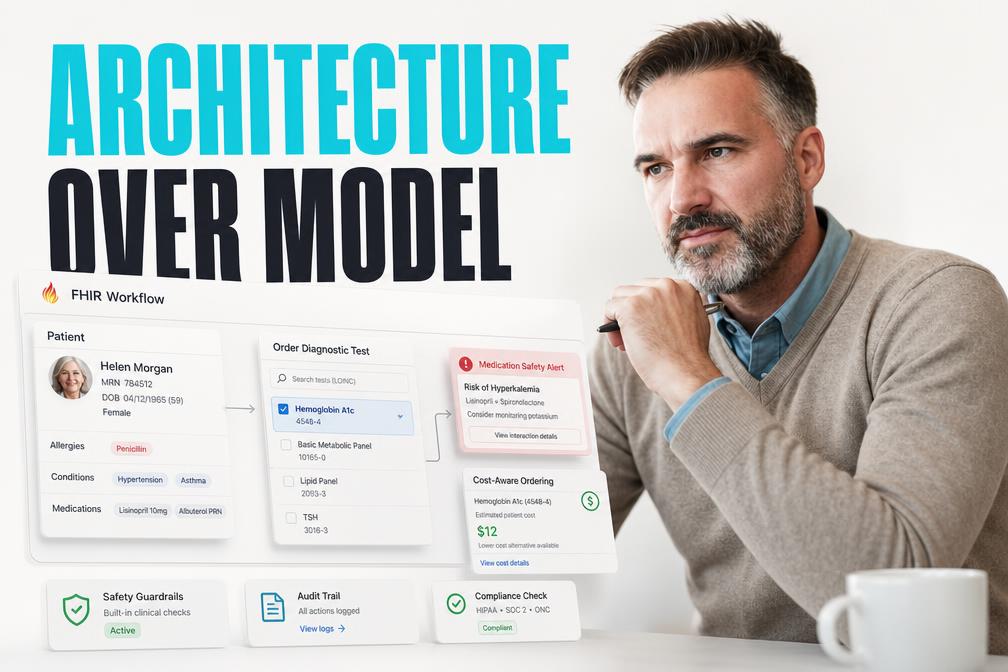
Why does the orchestration layer matter more than the underlying LLM? → The study shows that test‑selection strategy, FHIR‑based tool calls, and prescription validation drive performance, not just raw language‑model capability.
What should a healthcare CTO prioritize when piloting an autonomous agent? → Architecture integration, safety guardrails, and governance frameworks outweigh model selection in real‑world risk mitigation.
How can an organization move from sandbox success to production deployment? → By establishing a staged evaluation pipeline that validates workflow fidelity, resource utilization, and regulatory compliance before live rollout.
Quick Answer
Autonomous agents can reach physician‑level diagnostic accuracy in a sandboxed EHR, but their reliability hinges on integration architecture, safety guardrails, and human‑in‑the‑loop governance rather than on the raw model itself.
Why Diagnostic Accuracy Alone Misleads Healthcare AI Adoption
Diagnostic accuracy is a seductive metric because it is easy to benchmark against human performance. However, accuracy measured in a controlled sandbox masks the complexity of real‑world clinical workflows. In the MIRA experiment the agent could request any of 11 specialized digital tools, yet it deliberately avoided the over‑ordering of high‑cost imaging that typically inflates accuracy in retrospective datasets. This restraint emerged from a cost‑aware policy embedded in the orchestration engine, not from any intrinsic knowledge of radiology economics.
The hidden cost of a high‑accuracy model is the orchestration code that must enforce clinical guidelines, manage stateful interactions, and reconcile conflicting test results. When a model is deployed without such a layer, it can hallucinate test orders, generate unsafe medication regimens, or violate HL7 FHIR constraints – all of which would be catastrophic in a live hospital. Therefore, CTOs should treat diagnostic accuracy as a secondary KPI, focusing first on the robustness of the integration stack.
The Hidden Orchestration Layer in Clinical AI
MIRA’s architecture is built around a sandboxed FHIR server that records every tool invocation as a structured resource. Each request – whether to order a CBC, request a CT scan, or generate a medication order – is translated into a FHIR Procedure or MedicationRequest object, validated against a rule engine, and persisted for audit. This design provides two critical safety nets: (1) a deterministic audit trail that satisfies regulatory compliance, and (2) a deterministic gating mechanism that can reject unsafe actions before they reach the patient.
In practice, this means that the AI model outputs a high‑level intent (e.g., “order abdominal imaging”) and the orchestration layer resolves that intent into a concrete FHIR request, checking for duplicate orders, contraindications, and cost thresholds. The separation of concerns allows the language model to remain focused on reasoning while the orchestration code enforces policy. For engineering teams, this translates into a clear contract: the model must produce intent strings, and the middleware must enforce safety.
MIRA’s Architecture Shows Where Real‑World Integration Fails
The study’s sandbox replicated a realistic emergency department (ED) workflow, but it also highlighted gaps that would appear in production. First, the patient‑agent used in the simulation responded with perfectly structured clinical histories derived from retrospective notes. In a live ED, speech‑to‑text errors, incomplete histories, and patient anxiety introduce noise that can break intent extraction. Second, the sandbox’s FHIR server operated in isolation; a production EHR must interoperate with legacy modules, billing systems, and laboratory information systems, each with its own versioning quirks.
These gaps illustrate why many AI pilots stall after the proof‑of‑concept stage. Engineering teams must anticipate data heterogeneity, latency constraints, and backward compatibility when moving from a sandbox to a live EHR. The MIRA experiment suggests that a modular orchestration service, built on open standards like HL7 FHIR, reduces integration risk by providing a single, version‑controlled interface for all downstream systems.
Prescription Validation and Admission Decision Controls
Safety evaluations in the study revealed that MIRA produced zero high‑severity drug‑drug interactions, zero renal dosing incompatibilities, and zero medication‑allergy mismatches. The only shortfall was a 97% correctness rate for route specification, indicating occasional lapses in dosage form selection. This level of safety was achieved by embedding a prescription‑validation engine that cross‑checked every MedicationRequest against a curated drug interaction database and patient renal function data.
Admission decisions for pneumonia and pulmonary embolism were another focal point. MIRA achieved perfect recall for patients who required inpatient care, but it also displayed a tendency toward over‑admission for pulmonary embolism, reflecting a conservative risk‑averse policy. This pattern underscores the importance of calibrating decision thresholds: an overly cautious policy can inflate costs, while an aggressive policy can miss critical cases. CTOs must therefore design configurable safety policies that can be tuned to institutional risk tolerance.
What CTOs Must Prioritize When Evaluating Autonomous AI Agents
When a hospital leadership team asks whether to invest in an autonomous agent like MIRA, the decision matrix should be anchored on three pillars: (1) integration architecture, (2) governance and safety mechanisms, and (3) human‑in‑the‑loop workflows. Integration architecture determines whether the agent can speak the language of the existing EHR, retrieve lab results, and write orders without breaking HL7 FHIR contracts. Governance encompasses audit logs, policy engines, and compliance checks that prevent unsafe actions. Human‑in‑the‑loop workflows ensure that clinicians retain final authority over critical decisions, preserving trust and liability protection.
Choosing a vendor based solely on model size or benchmark scores is a false economy. Instead, evaluate the maturity of the orchestration platform, the extensibility of its rule engine, and the transparency of its audit trail. In practice, this means reviewing API specifications, examining how the system logs each FHIR transaction, and testing the configurability of safety thresholds before committing to a multi‑year contract.
Decision Framework: Architecture, Governance, and Human‑in‑the‑Loop
A practical decision framework begins with a technical feasibility study. Map the hospital’s current EHR interfaces – for example, the Cerner Millennium FHIR endpoint – against the agent’s required tool set. Identify any gaps, such as missing lab result APIs, and assess the effort required to bridge them. Next, construct a governance model that defines who can approve medication orders, how alerts are escalated, and what audit logs must be retained for regulatory review. Finally, design a clinician‑review workflow that surfaces the AI’s recommendations in the familiar EHR UI, allowing a physician to accept, modify, or reject each suggestion.
By iterating through these three layers, the organization can surface hidden integration costs early, avoid costly retrofits, and maintain a clear line of accountability. This approach aligns with the broader trend toward digital transformation that emphasizes composable services over monolithic AI deployments.
Business Impact of Deploying an Autonomous Clinical Agent
From a business perspective, the immediate value proposition of an autonomous agent lies in resource alignment. The MIRA study reported that the agent matched or exceeded physicians in overall resource‑alignment metrics, meaning it ordered fewer unnecessary high‑cost radiological studies while still achieving high diagnostic recall. For a hospital, this translates into lower imaging spend, shorter patient stays, and higher throughput in the ED.
However, the financial upside must be weighed against the cost of building and maintaining the orchestration layer, the ongoing need for clinical oversight, and the potential liability exposure if safety guards fail. A realistic ROI model should therefore include (a) savings from reduced test ordering, (b) revenue from increased patient turnover, (c) operational expenses for the integration platform, and (d) risk mitigation costs such as insurance premiums and compliance audits.
How to Pilot an AI Agent Like MIRA in Your Hospital
A pilot should be staged, beginning with a sandbox that mirrors the production FHIR profile. First, ingest a representative sample of de‑identified ED cases and run the agent end‑to‑end, capturing every FHIR transaction for audit. Second, validate the agent’s test‑selection logic against existing clinical pathways to ensure cost‑aware ordering. Third, introduce a clinician review interface that surfaces the AI’s recommendations within the live EHR, allowing a limited set of physicians to approve or reject each action.
During the pilot, track three core metrics: (1) diagnostic accuracy compared with ground‑truth chart review, (2) resource‑alignment efficiency measured by the ratio of ordered tests to clinically indicated tests, and (3) safety incidents captured by the prescription‑validation engine. A successful pilot will demonstrate parity or improvement on these metrics while maintaining a transparent audit trail.
Step‑by‑Step Evaluation Plan
The evaluation plan proceeds as follows. First, establish a secure FHIR sandbox that replicates the hospital’s production endpoints. Second, integrate the AI agent’s intent API with the sandbox, configuring the rule engine to enforce local formulary and imaging policies. Third, run the agent on a curated set of 200 de‑identified cases, recording every FHIR request and response. Fourth, convene a multidisciplinary review board – including physicians, pharmacists, and compliance officers – to assess safety outcomes. Finally, iterate on policy thresholds based on the board’s feedback before expanding the pilot to a live environment.
Real‑World Use Cases Beyond the Sandbox
While the study focused on emergency department triage, the same orchestration principles apply to chronic disease management, oncology treatment planning, and inpatient medication reconciliation. In a chronic‑care scenario, an autonomous agent could monitor longitudinal lab trends, trigger alerts for deteriorating biomarkers, and suggest medication adjustments, all while recording each action as a FHIR Observation and MedicationRequest. In oncology, the agent could orchestrate molecular testing, interpret genomic reports, and propose targeted therapy regimens, again leveraging a rule‑based safety layer to prevent off‑label prescribing.
These extensions illustrate that the value of a robust orchestration platform scales across specialties. By reusing the same FHIR‑centric middleware, hospitals can achieve economies of scale, reduce development effort, and maintain a consistent safety posture across disparate clinical domains.
Risks, Limitations, and the Road Ahead
The study also surfaces clear limitations. MIRA’s perfect recall for admission decisions came at the cost of occasional over‑admission, highlighting a bias toward safety that can increase inpatient load. The route‑specification error rate, though modest, indicates that even a well‑engineered rule engine can miss edge cases. Moreover, the simulated patient‑agent provided clean, structured histories, a condition unlikely to be replicated in noisy real‑world speech environments.
These risks suggest that full autonomy remains a few years away. Until the orchestration layer can robustly handle ambiguous inputs, integrate with legacy systems, and satisfy ever‑tightening regulatory standards, a hybrid model that couples AI reasoning with human oversight will remain the prudent path. Continuous monitoring, periodic re‑validation against live data, and adaptive policy tuning will be essential to maintain safety and efficacy.
Closing Insight
The MIRA experiment proves that autonomous AI can achieve physician‑level diagnostic performance when embedded in a disciplined, FHIR‑driven orchestration framework. For engineering leaders, the decisive factor is not how large the underlying language model is, but how rigorously the integration layer enforces clinical safety, resource stewardship, and auditability. By treating architecture as the primary lever, hospitals can unlock the efficiency gains of AI while preserving the trust and accountability that modern healthcare demands.
Explore how our AI agents development services can help you build a compliant, orchestrated AI platform. Our cloud software development expertise ensures scalable deployment, and our AI consulting team can guide you through governance and compliance.

